RAPID: The New Breakthrough Bargain

Is CMS Sending Mixed Signals?
Earlier this month, CMS looked like it was pulling back from Breakthrough Devices. In the FY2027 hospital payment proposed rule, the agency moved to repeal the alternative pathway for New Technology Add-On Payments and OPPS device pass-through payments for Breakthrough Devices. That pathway had allowed FDA-designated Breakthrough Devices to bypass the substantial clinical improvement requirement for supplemental payment. In my February Field Notes, I showed how significant that advantage had become: Breakthrough Device Designation was increasingly tied to NTAP success. Now, CMS says it has concerns with the limited evaluation process and wants all technologies receiving these payments to demonstrate that they substantially improve the diagnosis or treatment of Medicare beneficiaries.
Then, CMS and FDA announced RAPID, the Regulatory Alignment for Predictable and Immediate Device coverage pathway. RAPID is designed to accelerate Medicare coverage for certain FDA-designated Class II and Class III Breakthrough Devices, but that raises an obvious question. Isn’t that what NTAP, and more recently TCET (and before that MCIT), were all trying to do? Note: I know, that’s a lot of alphabet soup. I go into detail on each of these programs later.
The key difference, based on the announcement, is at what point acceleration happens. NTAP and pass-through payments operate after FDA authorization. RAPID appears to move the leverage point earlier. CMS would engage with FDA and manufacturers during development, align on Medicare-relevant clinical outcomes, and then issue a proposed national coverage determination the same day an eligible device receives FDA authorization. CMS says that could enable national coverage and payment as soon as two months after authorization, compared with roughly a year or more today. However, this still falls short of the automatic coverage the medtech industry has been lobbying for. In other words, RAPID may not make the path easier: it will require more time, more capital, and a higher Medicare-relevant evidence bar upfront, in exchange for a faster and more predictable path to coverage on the back end.
The Old Bargain Was About Launch Economics
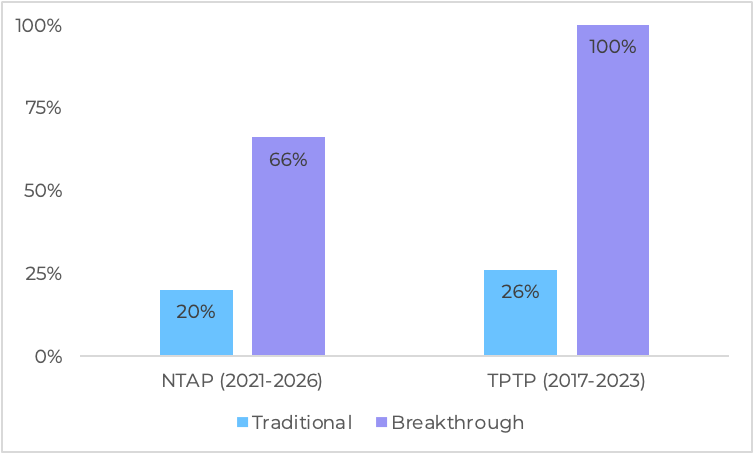
Previously, I looked at six years of NTAP data and found that Breakthrough designation had become much more than a regulatory tool. From FY2021 through FY2026, 76% of device applications that made it to the Proposed Rule phase also received Breakthrough designation, and 91% of successful NTAP awards came from Breakthrough applications. Breakthrough applications had a 66% success rate, compared with 20% for the traditional pathway. From 2024 through 2026, traditional device applications went 0 for 9.
That led to a pretty straightforward takeaway: NTAP had become the economic extension of Breakthrough. For founders, Breakthrough designation was no longer just about speed at FDA. It was becoming part of the reimbursement strategy. If NTAP was part of your launch plan, Breakthrough materially changed the odds.
That old bargain was mostly downstream: receive Breakthrough designation, get through FDA, and then use that designation to improve launch economics through NTAP. It helped answer one of the hardest early commercialization questions in medtech: how do we get paid at launch?
The Data Shows Why CMS May Be Recalibrating
The tension is that Breakthrough doesn’t necessarily mean the evidence base is mature. A study of Breakthrough device evidence at FDA approval (Kushal Kadakia, MD et al., JAMA Internal Medicine) found that Breakthrough Devices often move quickly through review, before the evidence base is fully built out (see Figure 1). These devices frequently rely on surrogate endpoints, limited follow-up, and post-market study requirements. That’s the point of the program: prioritize speed for technologies that could have significant patient impact. But it also means approval doesn’t necessarily signal a fully mature evidence base.
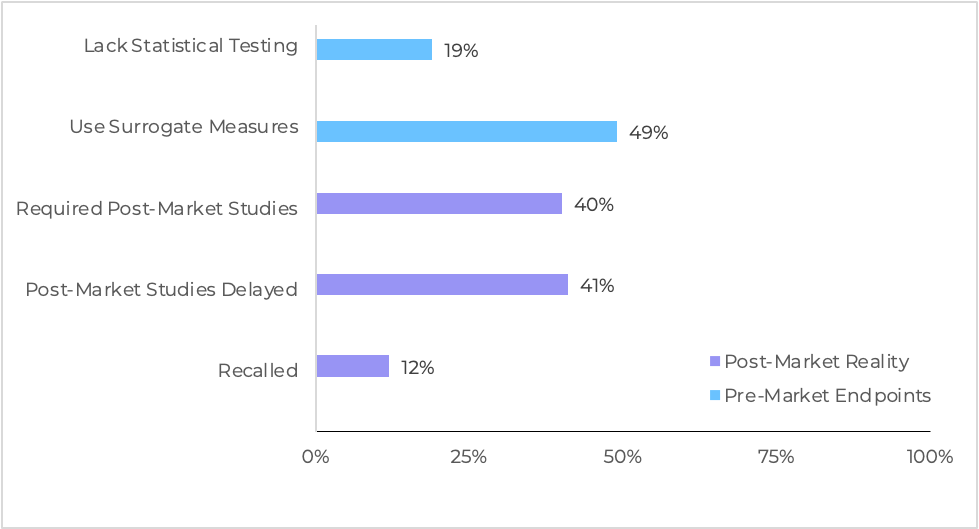
This distinction matters because FDA and CMS are typically answering different questions. FDA authorization asks whether a device is safe and effective for its intended use. Medicare coverage asks whether it is reasonable and necessary for Medicare beneficiaries. Supplemental payment asks something narrower still: whether the technology is new, costly, and represents a substantial clinical improvement over existing options. Those questions overlap, but they aren’t interchangeable.
The supplemental payment data points in the same direction (see Figure 2). In my NTAP analysis, 91% of successful awards came from Breakthrough applications. A study of outpatient pass-through payment approval patterns (Osman Moneer et al., JAMA Health Forum) shows a similar dynamic: all 8 Breakthrough applications for the Transitional Pass-Through Payment (TPTP) program were approved, compared with 9 of 35 through the traditional pathway. That is a significant difference, and it suggests the Breakthrough pathway changes the effective approval threshold for supplemental payment.
Another analysis by the same group adds an economic layer. Looking at manufacturer-reported versus observed hospital acquisition costs (Osman Moneer et al., JAMA Health Forum), researchers found that for Breakthrough Devices receiving supplemental reimbursement, manufacturers reported higher costs to CMS during NTAP or TPTP applications than hospitals ultimately paid, by a median of 9.7%. For 4 of the 18 devices studied, reported costs exceeded actual pricing by more than 50%. This gap between reported and realized pricing may help explain why CMS may be revisiting the program, particularly if reported costs are viewed as overstating real-world pricing.
RAPID Moves the Shortcut Upstream
RAPID is not simply a replacement for NTAP. Instead of relaxing Medicare’s payment review after authorization, RAPID appears to shift the leverage point earlier, into how evidence is generated. Based on early signals, CMS would engage with FDA and manufacturers during development, align on Medicare-relevant clinical outcomes, and use that alignment to accelerate coverage after authorization. To be eligible, a device must be a Breakthrough Device addressing unmet medical needs among Medicare beneficiaries, and must be studied in an IDE trial that enrolls Medicare patients and measures outcomes agreed upon by both FDA and CMS. That said, the details matter, and we will need to see how CMS and FDA formalize the program and what guidance ultimately looks like in practice.
This is the latest step in a multi-year effort to close the gap between FDA authorization and Medicare access. CMS initially attempted to guarantee coverage for all FDA-authorized Breakthrough Devices through the Medicare Coverage of Innovative Technologies (MCIT) pathway, finalized in 2021 but repealed before implementation. In 2024, CMS introduced the Transitional Coverage for Emerging Technologies (TCET) pathway, a more evidence-based approach that engaged with manufacturers before authorization and aimed to finalize coverage decisions within six months while allowing coverage during evidence development. In practice, TCET has been limited: capped at five devices per year, excluding diagnostics, and viewed as complex to navigate. CMS has now said TCET will be paused for new candidates as RAPID is implemented. RAPID appears to be CMS’s attempt to create something more scalable than TCET without reverting to the automatic coverage model of MCIT, with the potential to enable coverage and payment as soon as two months after authorization.
Next Steps for Founders
- Watch the Federal Register and consider commenting: A proposed procedural notice for RAPID will be published in the Federal Register, followed by a 60-day public comment period. CMS will respond to comments in a final notice, at which point the pathway is expected to take effect. Founders and other stakeholders should monitor closely and consider submitting comments, this is one of the few chances to shape how the program is implemented.
- Decide if RAPID is the right path for you: RAPID won’t be a fit for every company. In some cases, it may be more strategic to sequence studies and separate clinical/regulatory risk from reimbursement risk. RAPID will likely be most valuable when Medicare coverage is critical early and uncertainty around coverage is a gating risk.
- Budget for more evidence upfront: Meeting a higher evidentiary bar earlier will require more time, capital, and clinical complexity.
- Move reimbursement strategy upstream: the best-case RAPID strategy is a study that works for both FDA and CMS: Medicare-relevant patients, endpoints that support coverage, and early alignment on what evidence will count.
Taken together, this looks less like a policy reversal and more like a new evidence bargain. CMS is not saying every Breakthrough Device should automatically be covered. It is saying that coverage can move faster if the evidence is built differently from the start. If CMS helps define the target during development, the same evidence package used for FDA authorization may also support Medicare coverage.
For founders, that shifts the question. The new Breakthrough bargain is clear: meet a higher evidentiary bar earlier, often with more time and dollars in development, and you may be rewarded with faster, more predictable coverage on the back end.

